
[Updated 8/26/19, 10:30am. See below.] Remember when the new wave of expensive cholesterol-lowering drugs—known as PCSK9 inhibitors—was supposed to give the healthcare system a financial heart attack?
Far from it. Four years after approval the two PCSK9 blockers on the market have yet to crack $1 billion in annual sales, combined, thanks to a gloves-off effort by insurers to beat back their use. One of the two drugs might even be on life support.
Now a third PCSK9 inhibitor is in the ring. Results from a big study are due Sept. 2 at a medical conference in Paris. Wall Street analyst Umer Raffat of Evercore ISI recently called the presentation “one of the most important catalysts in the biotech universe.”
[Update: The drug’s owner, the Medicines Co. (NASDAQ: [[ticker:MDCO]]), released a preview of those results today, one week early. It did not release data, but the Medicines Co. (MedCo) said that the drug, inclisiran, met all its goals, mainly lowering LDL (bad) cholesterol by a significant amount, in the large Phase 3 study, ORION-11. MedCo said inclisiran’s safety performance was also “at least as favorable” as ongoing long-term studies. “We know the safety profile was super clean in prior trials,” Raffat wrote in a note this morning, “and safety was by and far the biggest issue heading into Phase 3.” MedCo shares are up 7.8 percent to $37.75 in morning trading.]
Still, with MedCo expected to push for marketing approval, the data that emerge next week will be important to demonstrate that inclisiran is at least as safe and effective as the first two PCSK9 fighters, but with an added weapon. The drug would be administered twice a year instead of self-injected under the skin every two or four weeks like the current drugs, evolocumab (Repatha) from Amgen (NASDAQ: [[ticker:AMGN]]) and alirocumab (Praluent) from Sanofi (NYSE: [[ticker:SNY]]) and Regeneron Pharmaceuticals (NASDAQ: [[ticker:REGN]]). MedCo has gone all-in for inclisiran, selling other products, cutting staff, and raising cash to pay for a series of trials, dubbed ORION. ORION-11, previewed today, is the first of the Phase 3 sections to report data.
MedCo has hinted at charging less than the current PCSK9 drugs but hasn’t revealed specifics, which will be crucial. When doctors convince insurers to pay for Praluent or Repatha, “patients are helped enormously,” says David Maron, director of preventive cardiology at Stanford Health Care in Palo Alto, CA. “But if inclisiran is significantly less expensive, there will be a big shift because it’s so much more convenient.”
What began as a story about the emerging power of genomics to find biomedical breakthroughs has, so far, turned into a healthcare hairball.
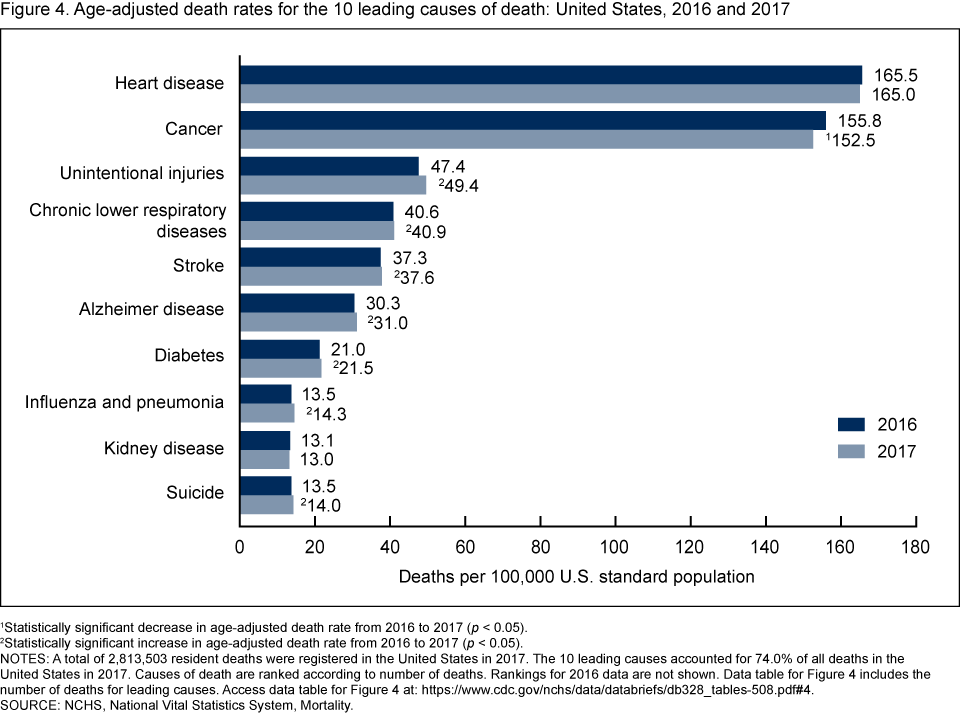
There’s little doubt millions of people need to lower their LDL cholesterol. Heart disease is the leading cause of death in the US and worldwide, despite the easy availability of generic cholesterol-lowering drugs called statins. PCSK9 inhibitors were approved in 2015 to help patients who can’t lower dangerous LDL cholesterol levels with statins and other drugs. But many cardiologists report prescribing Praluent or Repatha, only to be rebuffed by insurance companies, even after large studies published the past couple years provided evidence that PCSK9 blockers helped lower the risk of heart attacks and strokes.
{kind=link}
There’s always a challenge getting access to new drugs, says Prashant Vaishnava, a cardiologist at the Mt. Sinai Hospital in New York. (He has no ties to the PCSK9 companies.) “But I didn’t expect resistance to persist. It’s almost 2020.”
Insurers say they want to be sure patients are first maxing out on statins, for good reason. Many who should be on them aren’t, as studies like this one and this one have shown. “Statins are still the mainstay for treating cardiovascular disease,” says Norman Lepor, a Los Angeles cardiologist who has led large heart disease trials such as a recent high-profile fish-oil study. “But many of my colleagues are still undertreating patients.”
Statins only go so far, however. Many high-risk patients—how many is a matter of debate—have hit the maximum dose and still have high cholesterol, or they can’t handle the side effects. Lepor, who has earned hundreds of thousands of dollars in consulting and speaking fees from the PCSK9 drug makers, believes that because of high costs and bottlenecks to deny PCSK9 coverage, “lives were lost.” A recent study in the journal Circulation backs him up. (It was conducted by a nonprofit group, the FH Foundation, which advocates for people with genetically high cholesterol levels; the foundation takes pharmaceutical payments.) An accompanying editorial in the journal also chides companies for high prices that block access “for the most vulnerable segment of our society.”
Denied coverage
An earlier study in Circulation, published in late 2017, showed 53 percent of PCSK9 inhibitor prescriptions were rejected by insurers in the first year of the drugs’ availability. Lepor and other doctors say anecdotally the bottleneck seems to have eased after recent price cuts and evidence of lives saved. (According to data from IQVIA and SVBLeerink, total combined prescriptions for Praluent and Repatha have grown slowly since launch, only recently passing the 25,000 mark, well short of estimates of potential eligible patients.)
Doctors aren’t satisfied. They report that unreasonable denials are still happening. Here’s one recent case: A patient at Maron’s Stanford clinic, who asked not to be named, is a Northern California man in his 30s with a family history of heart disease. He has had sky-high LDL cholesterol from childhood, a sign that it’s a genetic condition. Statins only brought his LDL cholesterol down to about 100. He says cannot take another generic cholesterol fighter, ezetimibe, because of side effects. He hasn’t had a heart attack or stroke yet, but he feels the urgency to lower his LDL level to 50 or 75, having already had a lifetime of arterial damage. Maron recently prescribed him a PCSK9 inhibitor.
Maron says his staff has done well getting authorization for PCSK9 inhibitors, but not this time. The insurer won’t pay for it. “It makes me angry,” says Maron, who calls the denial a “lack of response and responsibility to a legitimate need for my patient.” (Maron is co-chair of a closely watched National Institutes of Health cardiovascular study that has some support from Amgen but otherwise reports no ties to the PCSK9 companies.)
The insurer, Aetna (NYSE: [[ticker:AET]]), requires five conditions to cover the PCSK9 inhibitor Repatha. Its denial-of-coverage letter said the patient did not meet all five, but it did not specify which ones. When asked for details, an Aetna spokesman sent Xconomy a statement that said, in part, “an individual is required to fail two different statins before being approved for Repatha or Praluent.” Aetna said that Maron had confirmed “that [the patient] had not met the criteria at the time.”
Aetna said the patient has the right to appeal.
Shown Aetna’s statement, Maron responds bluntly: “Not true.” The patient did, in fact, try two different statins before Maron prescribed the PCSK9 inhibitor, Maron says. What’s more, he says, Aetna’s statement to Xconomy doesn’t line up with what Aetna previously told Maron’s staff: “Our nurse practitioner, who appealed the denial, was told by Aetna that he did not meet criteria due to lack of physical findings (xanthomas) and lack of clinical coronary disease in himself or in a first degree relative, and because his genetic testing for familial hypercholesterolemia was negative.”
It’s true that the patient had a negative DNA test, but a negative test doesn’t rule out the condition. Only a positive test can rule it in. Maron says that after the denial he tried reaching Aetna through an appeals line, but his messages were never returned.
Payer resistance eventually forced Amgen and Regeneron to slash prices nearly 60 percent in the past year, from more than $14,000 a year to less than $6,000 a year. (The drugs must be taken for life to keep high cholesterol at bay.)
Repatha brought in $550 million in 2018. Praluent tallied about $300 million. Both fall short of expectations. Even a skeptic of their market power predicted back in 2014, prelaunch, that 2019 sales would top $1 billion for each. Wall Street analysts were much more bullish.
The companies hope they can ramp up prescriptions to make up for the price cuts. In the first half of 2019, Repatha revenues were practically equal to the second half of 2018. But the company reported that US prescriptions filled (that is, approved by insurers) grew 66 percent in the second quarter over the same period in 2018. Amgen’s executive VP of global commercial operations Murdo Gordon said on the quarterly call in July that Amgen is “disappointed” about restrictions of the lower-priced Repatha under Medicare, despite the price cuts, and will try to crack that market in 2020. “We expect that we will see a positive impact on volume and reported net sales growth over the long term,” he said.
On Regeneron’s quarterly earnings call August 6, CEO Len Schleifer said the company and its partner Sanofi would “stem losses from Praluent by better aligning investments with revenues.” An analyst wondered aloud if the partners might “take a tough personal decision” about Praluent, or if they could turn it around to profitability. Schleifer responded with a less-than-rousing defense: “Obviously, this is a highly competitive space. And we don’t want to get too detailed about what our strategies are. We said we’re trying to match our investments appropriately, but we do have some strategies. At the end of the day, heart disease is still a major killer. The PCSK9 [inhibitor] is still a terrific drug. So maybe that’s all we should say at this point.”
A Regeneron spokesman declined to elaborate upon Schleifer’s comments or discuss Praluent prescription data.
Here comes inclisiran
PCSK9 (proprotein convertase subtilisin/kexin type 9) is made in the liver. Too much of it hinders the body’s ability to clear bad (LDL) cholesterol from the blood. Repatha and Praluent are engineered antibodies that latch onto excess PCSK9 so it can be flushed out of the body. Inclisiran goes right to the source, entering liver cells and preventing them from making PCSK9.
The science behind the drug is called RNA interference, or RNAi. The discovery that the interruption of RNA, the molecular carriers of DNA instructions, could block the production of a protein—like shooting down a messenger pigeon—won a Nobel Prize in 2006. The first RNAi drug came to market just one year ago.
That drug’s owner, Alnylam Pharmaceuticals (NASDAQ: [[ticker:ALNY]]), also discovered inclisiran. It sold rights to the Medicines Co. in 2013, a deal Alnylam’s CEO told Xconomy in 2015 he would like to redo after Alnylam’s drugs began to show signs of lasting for months via a single injection.
Under MedCo’s guidance, inclisiran has hit its marks and then some. Biotech analyst Raffat said a peek at long-term data earlier this year “might constitute one of the largest safety follow-ups we’ve seen in the RNAi space, and safety looks very good.”
Inclisiran also reduced bad cholesterol 51 percent in that long-term study, putting it on par with Repatha and Praluent. Two big hurdles remain. The first is next week’s first reveal of Phase 3 data. If inclisiran bolsters earlier results from smaller studies, as MedCo announced today, the company will push toward approval and launch within two years. There could be more competition by then. Two pills from Michigan’s Esperion Therapeutics (NASDAQ: [[ticker:ESPR]]), which taken daily would help lower LDL cholesterol in people already on statins, are under FDA review and could be approved early next year.
But as Amgen, Regeneron, and Sanofi have learned, the bigger hurdle in this space is the support of payers. Cost and convenience will be a delicate needle to thread. MedCo’s previous CEO has talked about inclisiran as a high-volume, lower-cost product: a cholesterol injection for the masses. For that to happen, the upcoming Phase 3 safety data will have to be pristine.
Asked about pricing and payers, MedCo spokesman Michael Blash wouldn’t give specifics but said inclisiran has “a vastly different value proposition compared to any other LDL-C lowering option” and “the potential to change the landscape of cardiovascular treatment.” “We’re less than two years from expected launch,” Blash said, and conversations with payers and others have reinforced the firm’s confidence.
Leading up to their approval, Repatha and Praluent inspired confidence and lofty language, too. Even if inclisiran’s upcoming results are as good as the previous ones, and regulators are swayed, payers might not be. MedCo has begun a study to show, as Amgen and Regeneron did, that their PCSK9 blocker prevents heart attacks, strokes, and other cardiac events. That study, ORION-4, aims to enroll 15,000 people with a median follow-up of at least four years.
Amgen’s 27,000-person Fourier study reported a modest overall benefit in reducing cardiac events like heart attack and stroke but did not last long enough to show a boost in survival. Regeneron’s 19,000-person Odyssey Oucomes study reported a similar risk reduction for cardiac events but added a potential reduction in the risk of death for patients who had previously had a heart attack or stroke. (The risk-of-death data, however, were not statistically significant for all patients.)
Inclisiran’s outcomes study is expected to end in 2024. MedCo plans an interim peek at the data before then, says Blash, but declined to be more specific. When announced, that date will be circled on a lot of calendars. “I doubt access will be easy, having seen the experience with the other PCSK9 inhibitors,” says Mt. Sinai cardiologist Vaishnava, who also urges some perspective. “It’s important to not lose sight of the basics, step back and make sure patients remain on statins and aspirin. Just be mindful that it’s not all about using the latest and greatest medicines.”
Image courtesy of the University of Liverpool Faculty of Health and Life Sciences via Creative Commons. (Image was altered from the original.)